







Ceramics are widely used in dentistry due to their ability to mimic the optical characteristics of enamel and dentine, as well as their biocompatibility and durability. They include a wide array of materials.
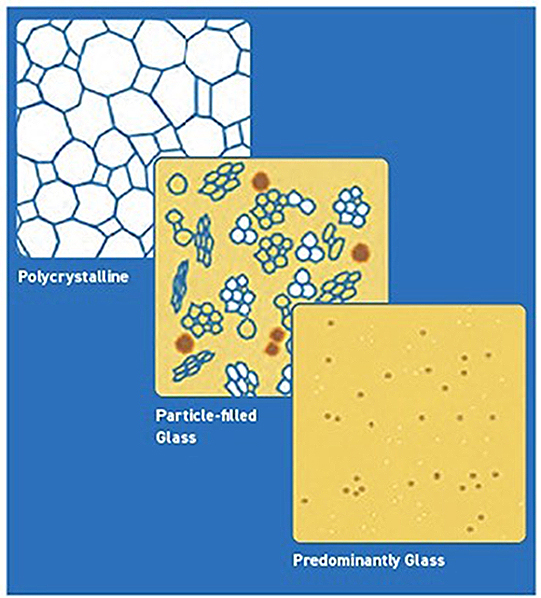
There are three main classes of dental ceramics: predominantly glassy materials, particle-filled glasses, and polycrystalline ceramics (See Figure 1). In general, the higher the proportion of polycrystalline components, the higher the strength of a ceramic.
Conventional production involves blending the minute particles of raw material, forming the mixture into a green body, and firing it at a high temperature. This process is referred to as sintering, which fuses the individual grains to produce a hard, durable, corrosion-resistant product.
Tooth tissue loss is caused by caries or traumatic injuries and might be prevented. However, surface loss due to aging is unavoidable. It is the result of tooth interaction with an opposing tooth, the food that is being chewed, and even the toothbrush and toothpaste. Besides numerous advantages of dental ceramics such as superior aesthetics, favorable physical and mechanical properties, and biocompatibility, these materials might be a factor in additional tooth-surface loss. The quantity of surface reduction depends on the ceramic material (chemical composition and microstructure), final procedures before cementation (glazing, finishing and/or polishing), and the restoration type (inlay versus overlay or full crown).
Tooth surface loss
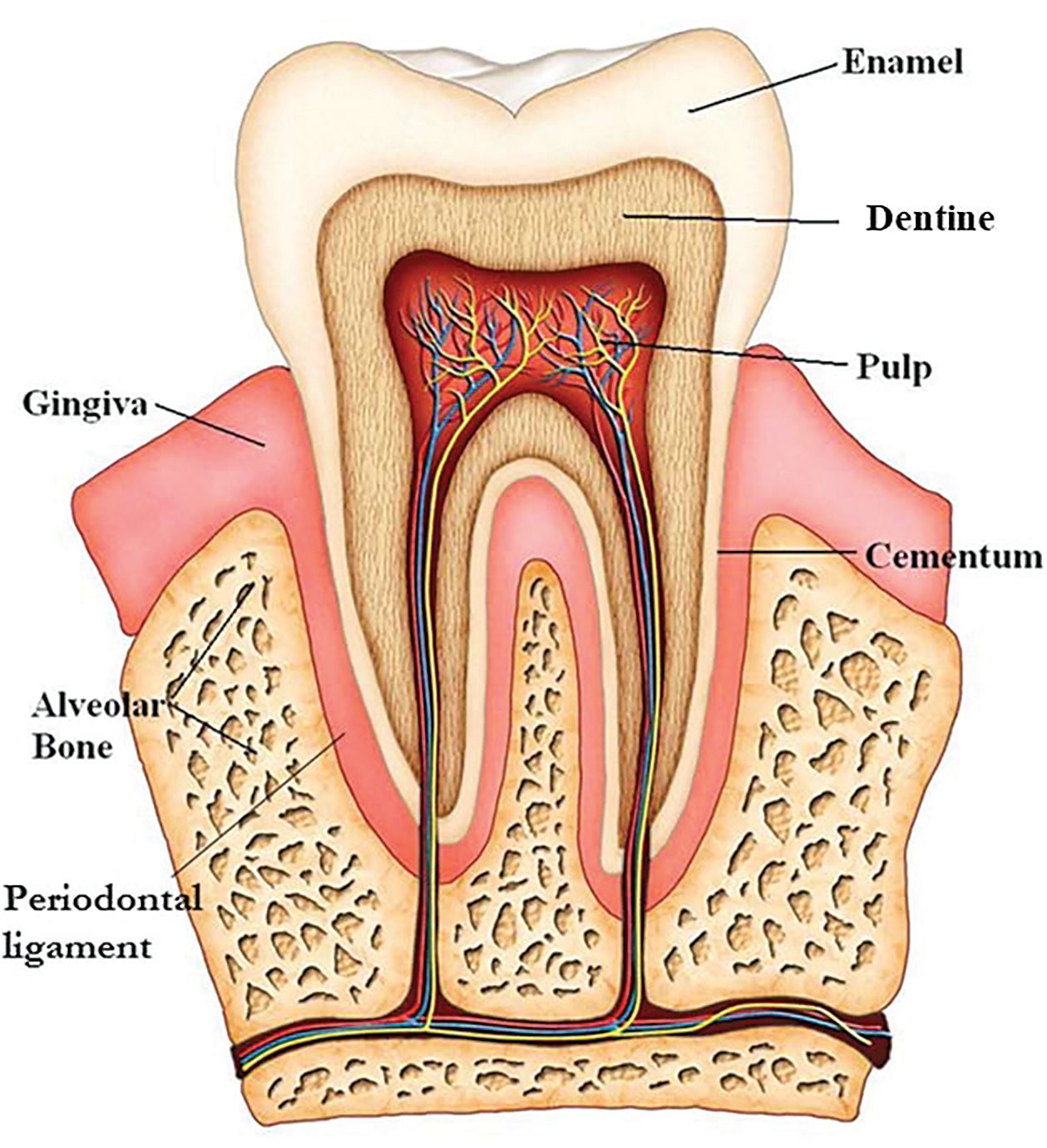
Tooth surface loss most often results from natural tooth-to-natural tooth and/or natural tooth-to-restoration contact (See Figure 2). It is often accelerated by restorations — this is especially true with opposing ceramic restorations. The reduction of surface might lead to a variety of problems. These include loss of enamel, loss of dentine, teeth fracture, hypersensitivity, compromised aesthetics, misshapen teeth, loss of tooth vitality, and problems in chewing and possible jaw problems as a result of reduced facial vertical dimension in patients with generalized tooth surface loss (See Figure 3).

This tooth surface loss can be categorized as:
- Erosion (loss due to acids).
- Attrition (loss due to tooth-to-tooth contact).
- Abrasion (loss due to contact with a foreign object such as a toothbrush).
- Abfraction (loss due to flexure, i.e., fatigue cracking).
Tooth surface loss is usually a result of a combination of these factors — with abfraction often instigating the process.
Lab tests reveal that the following factors have a strong influence on the extent of wear:
- Configuration (more wear of flat surface).
- Surface treatment (more wear of glazed versus polished restorations).
- Antagonist system (more material wear and less antagonist wear for ceramic versus enamel) [1].
- Enamel thickness (more wear with thinner enamel).
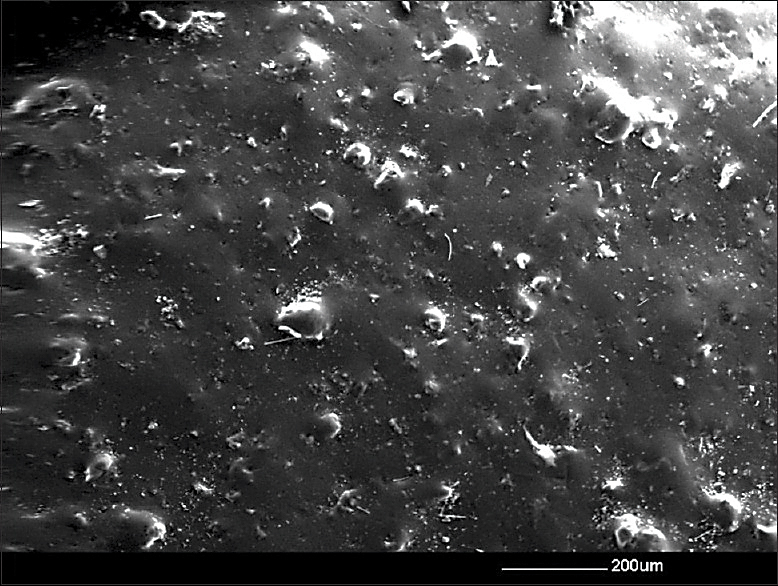
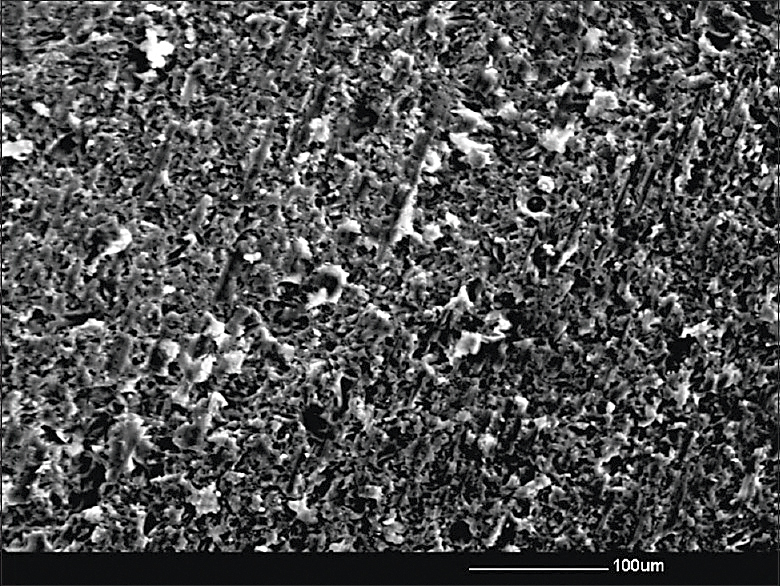
The surface finishing and contouring of ceramics does have a significant effect on the rate and extent of wear (See Figure 4). However, ceramic restorations when polished are hard on opposing enamel and on opposing natural teeth that have restorations. Ceramics, while aesthetically favorable and very wear resistant in themselves, are even more abrasive than gold, amalgam and composites. This is one of the reasons dental professionals don’t favor ceramics in all applications (See Figures 5 and 6).
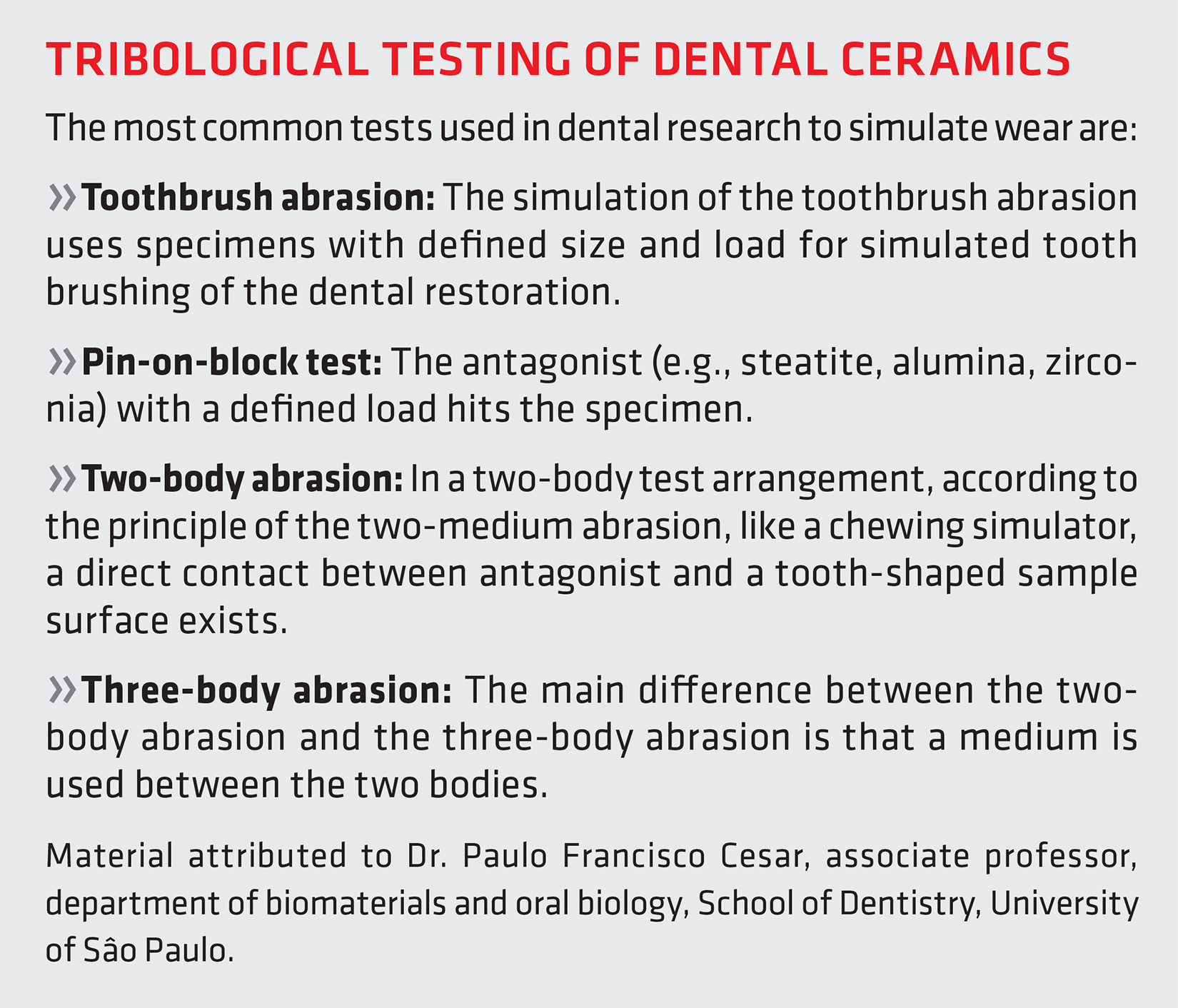
“In general, the wear of brittle materials, such as dental ceramics, occurs primarily due to crack growth mechanisms rather than plastic deformation,” said Dr. Paulo Francisco Cesar, associate professor, department of biomaterials and oral biology, School of Dentistry, University of Sâo Paulo. “Factors that influence the wear behavior of dental ceramics include ceramic type, microstructure, fracture toughness, surface quality/roughness, contact load, environment, and the number of cycles. Wear facets in dental ceramics usually present a series of superficial microcracks forming a zone of quasi-plastic deformation.” [2]
Cesar goes on to explain that, under higher contact loads and high friction, subsurface crack propagation (brittle fracture) results in the formation of large wear particles due to delamination. Delamination wear of glass ceramics is associated with the presence or formation of microcracks. Because of this, ceramic materials that possess higher fracture toughness, such as zirconia, are able to resist delamination wear better than low-fracture toughness ceramics, such as porcelain, that possess lower fracture toughness [3].
In vitro wear studies have revealed partially detached wear particles and/or subsurface cracks running parallel to the sliding surface in both dental ceramics and enamel. These indicate that the wear particle formation can occur gradually with a lateral crack extending due to cyclic tensile loading by the sliding antagonist (i.e. delamination wear controlled by a fatigue process). The delamination process can, thus, result in relatively low wear or high wear, for example, when considering enamel opposing polished zirconia under low load or enamel opposing rough zirconia under high load, respectively.
“Overall, lower ceramic and/or opposing enamel wear is generally noted when the ceramic material possesses high flexural strength or fracture toughness, the ceramic material, particularly for feldspathic porcelains or leucite glass ceramics, contains a high fraction of small, uniformly distributed crystals, when the ceramic contains fewer internal defects (e.g., cracks, pores) or the surface roughness of ceramic is reduced (e.g., by polishing),” Cesar said.
Maximizing durability
“Efforts to understand clinical failure of single crowns and multi-unit prostheses (bridges) has involved studying fracture surfaces from clinically failed prostheses (using fractography), finite-element analysis modeling, and developing clinically valid laboratory tests,” said J. Robert Kelly, DDS, MS, DMedSC, professor of prosthodontics and dental materials science, School of Dental Medicine, University of Connecticut Health. “These all demonstrate that the main mechanism of bulk failure of single ceramic crowns does not involve damage from wear facets but stresses on the cementation surface due to occlusal loading.”
According to Kelly, there are four clinical techniques for maximizing durability:
1. Providing maximum occlusal thickness for the ceramic (strength increases with the square of the thickness).
2. Using the highest elastic modulus (stiffness) substrate possible (i.e., metal or ceramic versus resin-based composite).
3. Bonding the restoration, ceramic cement, and cement tooth (or substructure).
4. Developing broad, not pinpoint, occlusal contacts.
 Advancements in ceramics
Advancements in ceramics
“Dental ceramics is a unique family, not only due to the varieties in the physical and mechanical properties but also due to the variation in the production methods and uses,” said Dr. Ahmed Hussain, assistant professor in prosthodontics at the College of Dentistry, University of Saskatchewan. “Initially, dental ceramics were composed mainly from materials that exist in nature such as silica, potassium, sodium and others — glass-based ceramics. Although they are still in use due to their high aesthetic characteristics, they have low flexural strength, which makes them unsuitable for use in the high loading areas of the mouth. That is why their use is usually limited to the anterior part of the mouth.”
“Later on, high-strength ceramics such as zirconia were introduced,” he said. “Although zirconia has a high flexural strength, its aesthetic characteristics are not close to that of the glass-based ceramics. So, the dentist sometimes uses a combination of ceramic materials to address the functional and the aesthetic needs of the patient.”
All ceramic materials have excellent aesthetic qualities that rival healthy natural teeth. However, ceramics tend to be brittle and fracture under high stress. To offset that, the current trend is to reinforce ceramics with crystalline materials. There are three basic categories of dental ceramics:
- Predominantly glassy (also called porcelains).
- Particle-filled glasses.
- Polycrystalline.
Kelly explains these three categories as follows:
• Predominantly glassy ceramics are based on feldspar, are resistant to crystallization (devitrification) during firing, have long firing ranges (resist slumping if temperatures rise above optimal) and are extremely biocompatible. In feldspathic glasses, the 3D network of bridges formed by silicon-oxygen-silicon bonds is broken up occasionally by modifying cations such as sodium and potassium that provide charge balance to non-bridging oxygen atoms.
• Particle-filled glasses have filler particles that are added to increase the strength and fracture toughness of the ceramic. Commonly used fillers include aluminum oxide, leucite, and lithium disilicate. These particles can decrease the natural flaw size of the ceramic and make crack initiation and propagation more difficult. They also generally increase the opacity of the ceramic as well by increasing light scatter.
• Polycrystalline ceramics have no glassy phases; all of the atoms are densely packed into regular arrays that are much more difficult to drive a crack through than atoms in the less dense and irregular network found in glasses. Hence, polycrystalline ceramics are generally much tougher and stronger than glassy ceramics. Well-fitting prostheses made from polycrystalline ceramics were not practical prior to the availability of computer-aided manufacturing.
According to Kelly, the dental ceramics that best mimic the optical properties of enamel and dentin are predominantly glassy materials (see Tribological Testing of Dental Ceramics).
 Processing
Processing
Porosity in dental restorations is undesirable because it increases the roughness of the surface and can lead to increased wear. Sintering reduces porosity. During the sintering process, high heat causes the ceramic particles to consolidate. This leads to a reduction in the porosity of the surface and, to some degree, the rest of the material. The extent of porosity depends on the length of time and the degree of temperature during the sintering process.
Porcelain can be fortified via a process called “dispersion strengthening” during which the material is reinforced with magnesia and alumina. Zirconia also can be added to strengthen the porcelain in a process called “transformation toughening.” When the zirconia is further stabilized with yttria (yttrium oxide), it has increased strength, thermal shock resistance, and fracture toughness. The downside is that it is less translucent. Because of this, copings are usually veneered to achieve better aesthetics.
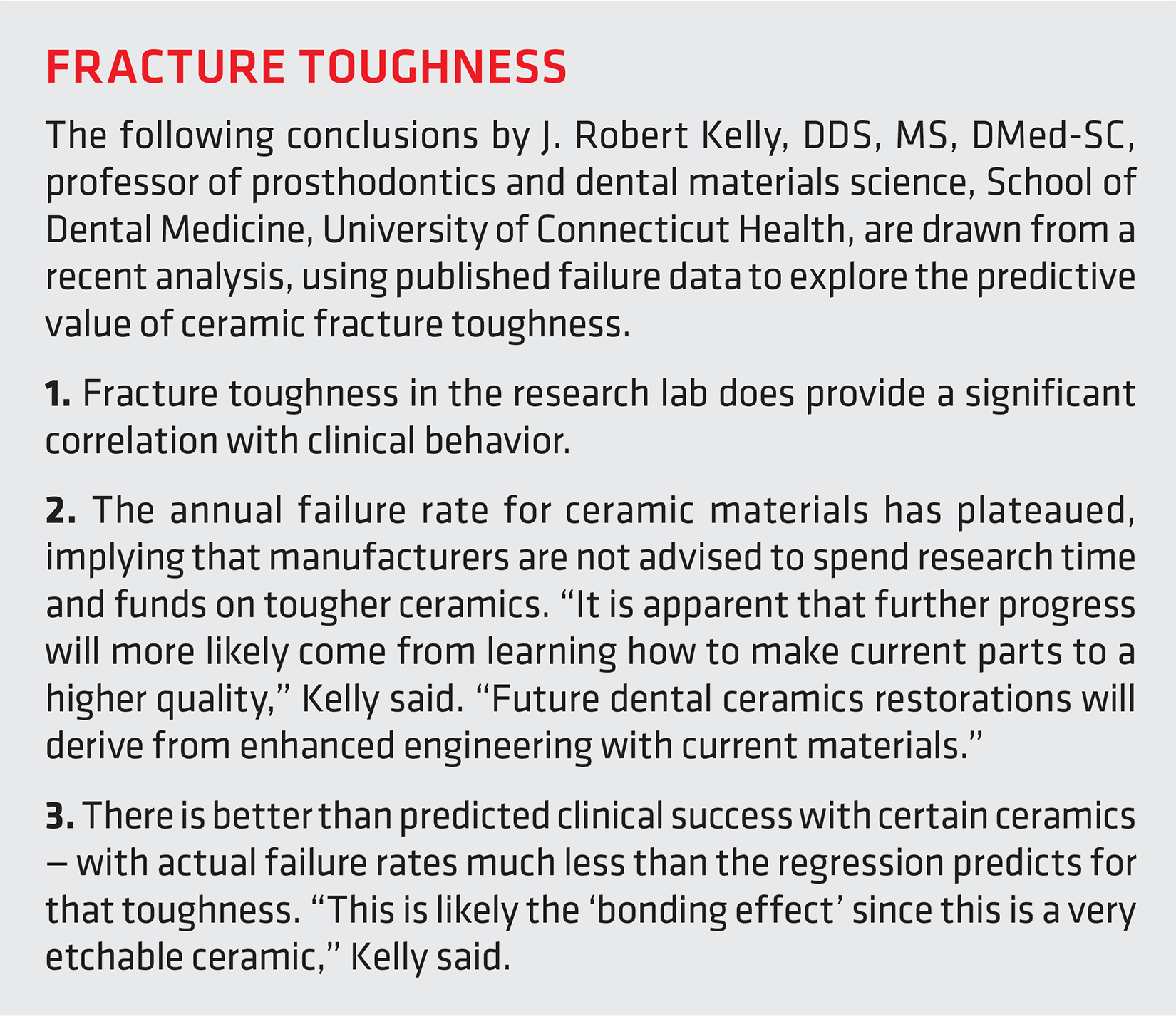
Glass ceramic restorations are developed in a non-crystalline state and then converted into a crystalline material. To fabricate glass ceramic restorations, wax patterns are made using a dental wax. The liquefied ceramic is cast into the empty space in the investment material after the wax has been burned out. Then the glass is heated again for six hours. This leads to the formation of tetra-silicic fluoromica crystals. The resulting crystals improve strength and fracture toughness and increase abrasion resistance and chemical durability (see Fracture Toughness).
 “The ceramic material itself does not affect the price of the dental restoration significantly,” Hussain said. “The major factor that would affect the price is the time required to fabricate the restoration, the experience of the ceramist and (the more the experienced the ceramist, the higher the fee) if it is going to be fabricated either partially or completely by computer-aided manufacturing or if it will be fabricated the conventional way.”
“The ceramic material itself does not affect the price of the dental restoration significantly,” Hussain said. “The major factor that would affect the price is the time required to fabricate the restoration, the experience of the ceramist and (the more the experienced the ceramist, the higher the fee) if it is going to be fabricated either partially or completely by computer-aided manufacturing or if it will be fabricated the conventional way.”
Most dental professionals are aware of not just these and other recent advancements in ceramic restorative materials but also the importance of finishing and polishing these materials before finalizing the patient’s procedure.
“In dental prosthodontics, the surface finish is a key factor,” Cesar said, “Finishing and polishing can be carried out intraorally or in the laboratory. Intraoral polishing is a difficult task and demands good operator skills and a variety of intraoral instruments to achieve an acceptable result. The final aim in dentistry is to achieve the lowest surface roughness possible, as rough surfaces result in more wear, more biofilm accumulation and discomfort for the patient.”
Advancements in manufacturing
The development of computer-aided design/manufacturing (CAD/CAM) methods for the creation of restorations such as inlays, crowns, and bridges has enabled cutting-edge machinable ceramics. Because they can be created while the patient is still in the chair, they eliminate at least one additional visit. The downside is that CAD/CAM technology is expensive, and the process requires more than a little expertise.
“Technological improvements have come from both design/processing and materials enhancements (See Figure 7),” Kelly said. “Understanding how to maximize durability by design and processing flows from understanding clinical failure and the factors influencing the stress state at failure that are within our clinical control. (See Figures 8 and 9)



CAD software sets the parameters for the dimensions and shape of the restoration; CAM software defines and governs the manufacturing process. CAD/CAM has been used for restorations by dental professionals for three decades. Prior to that, the alternative was slip-casting, which resulted in more defects/cracks in the restoration.
CAD/CAM systems are continually producing better restorations, for not only ceramics but also metal alloys and resin composites. CAD/CAM techniques for producing restorations involve:
- Machining the prosthetic restoration from a mass of sintered material.
- Machining a partially sintered mass that then requires final sintering.
- Additive manufacturing technique (AMT).
The first method results in a more precise restoration and also takes less time. However, with some materials, it can lead to defects, be hard on the machining unit, and actually take more time.
The second method has the advantage of healing defects that occurred in the machining process during the subsequent sintering process. This final sintering, however, can misshape the restoration and create a misfit in the patient’s oral area. One of the issues with CAD/CAM for dental restorations is that the machining process wastes about 90 percent of the material, which cannot be reused. New technologies are being developed to mitigate this such as AMT [4].
“Usually dental ceramics can be produced either conventionally or digitally,” Hussain said. “In the conventional method, the quality of the final restoration is highly dependent on the technique, the material used, and the experience of the dental technician. The conventional method is usually time consuming, and it is getting less common in dental labs because of the advances in digital technology. More dental offices are getting digital scanners to scan the prepared teeth. Then they send the digital files from the scanners to the lab. In the lab, a dental technician, with the help of special software, can fabricate a restoration that will not only fit the prepared teeth but provide function, aesthetics, and comfort for the patient.”
Hussain believes digital restoration design software is an essential part of any dental lab because more dental clinics are sending their impressions digitally—today many restorations are completely designed and fabricated digitally. This includes anything from a single restoration up to a full mouth restoration. Hussain said digitized manufacturing has improved dental ceramics in the following ways:
- It has reduced the time of dental restoration production.
- It has reduced the cost.
- It has led to better quality consistency since the material is supplied by the manufacturer in the processed or green stage.
- There are better physical and mechanical properties of the materials.
- The production of such materials as high-strength ceramics is much easier.
- A replacement restoration can be fabricated because the file for the restoration manufacturing is already stored digitally.
- There is less possibility for error since there is less of a human factor involved in production.
“The digital revolution has radically changed the workflow in dental clinics around the world, and some dental ceramics like zirconia are only produced via CAD/CAM,” Cesar said. “Gradually, prosthodontic procedures are changing to a completely digital workflow, beginning with the planning steps that include printing test-drive smiles in a 3D printer, with subsequent planning of the rehabilitation in an advanced CAD software and final steps involving milling the ceramic restoration in specialized CAD units. By using this workflow, a full-mouth rehabilitation with ceramics can be performed in two or three days.”
Aesthetic considerations
There are several factors that affect the aesthetics of the dental restoration such as optical properties, surface texture, polish ability, resistance to staining, and color stability. The missing tooth structure is usually composed of two layers (dentin and enamel). The combination of these two layers affects the tooth value, color, and chroma.
“A closer look at the complex light interaction with these two layers makes us wonder if there is a single ceramic material that can have aesthetic properties similar to the natural tooth structure,” Hussain said, going on to explain that the dentist usually faces one of the following two scenarios:
• The dentist is trying to restore a non-discolored tooth for a patient who does not want to change the color of the tooth but to improve its shape or restore the missing tooth structure. “In this scenario, the dentist should try to use a ceramic material that has a high translucency so that the light can pass easily through the restoration to interact with the natural tooth structure, which, in turn, will show the natural color of the tooth,” Hussain said.
• The dentist is dealing with discolored teeth that the dentist and the patient both think are undesirable. In this scenario, the dentist should use a high opacity (low translucency) dental ceramic to block the undesired color of the tooth and to establish a new natural color.
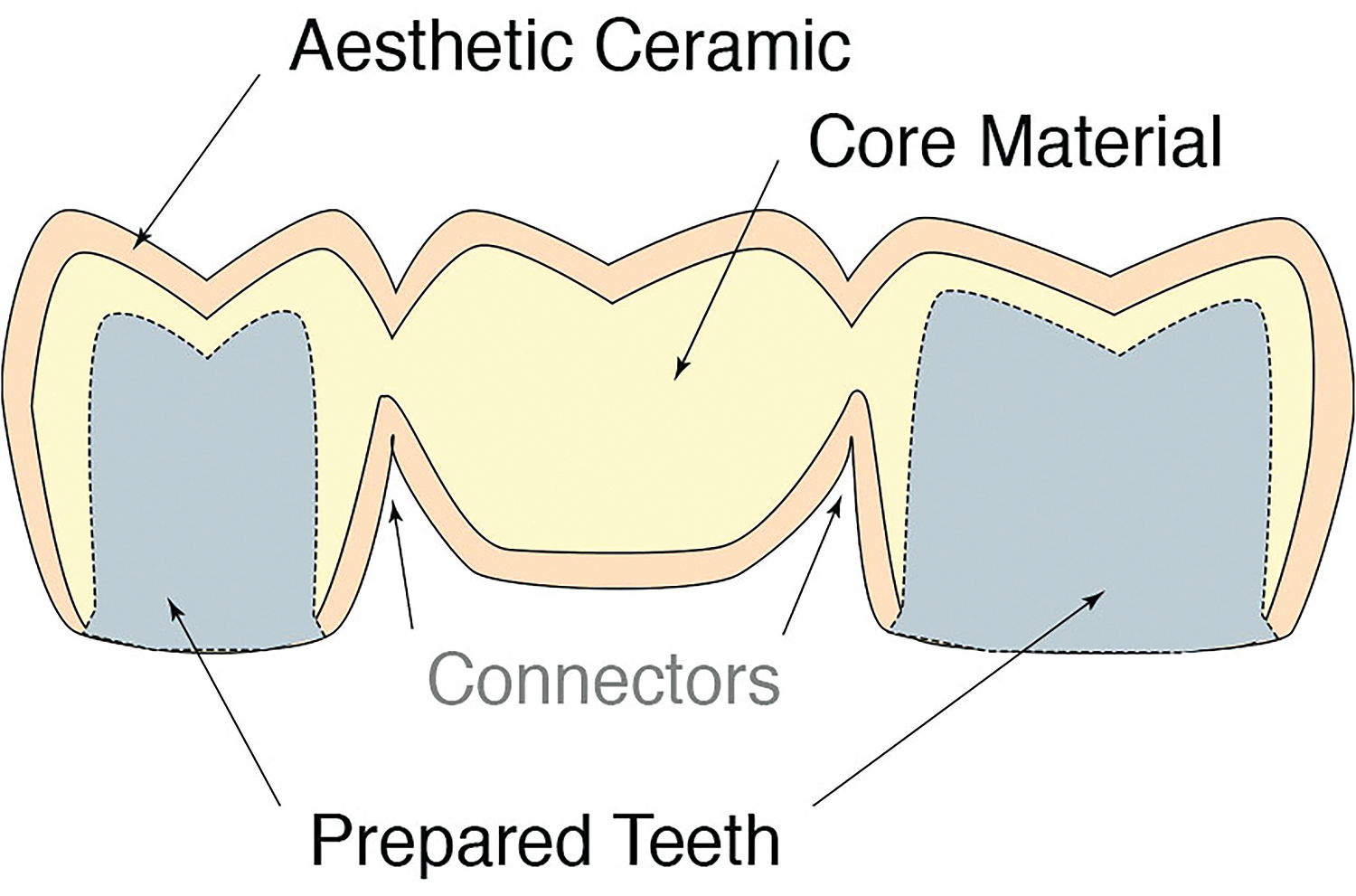
As ceramic materials and processes continue to develop, aesthetics, wear resistance, and patient convenience will improve (See Figure 10). “Twenty years ago, I would not have predicted the use of engineering failure analysis of clinically failed prostheses and the increased use of clinical longevity studies to improve the performance of dental ceramics,” Kelly said. “However, design details, such as crown thickness and connector dimensions of multi-unit prostheses, have derived from these investigations.”
References
- An antagonist tooth is in the opposite arch against which a tooth occludes.
- Kruzic, J.J., Arsecularatne, J.A., Tanaka, C.B., Hoffman, M.J. and Cesar, P.F.J. (2018), “Recent advances in understanding the fatigue and wear behavior of dental composites and ceramics,” Journal of the Mechanical Behavior of Biomedical Materials, 88, pp. 504-533. DOI: 10.1016/j.jmbbm.2018.08.008. Epub: 2018 Aug.
- Porcelain is a subset of ceramics. The two terms are not synonymous, though sometimes used that way.
- Dental ceramics: A review of new materials and processing methods. Available at https://www.scielo.br/j/bor/a/nqvZnkdKr9synf4bjFr5wPk/?format=pdf&lang=en.
About the author
Jeanna Van Rensselar heads her own communication/public relations firm, Smart PR Communications, in Naperville, Ill. You can reach her at jeanna@smartprcommunications.com.
Reprinted with permission from the November 2020 issue of TLT, the official monthly magazine of the Society of Tribologists and Lubrication Engineers, an international not-for-profit professional society headquartered in Park Ridge, Ill., www.stle.org. Available at https://www.stle.org/files/TLTArchives/2020/11_November/Feature.aspx.



















 general practice for CQI-9 and AMS2750E")





